

Understanding Attachment
Early Bonds, Safety & Emotional Development
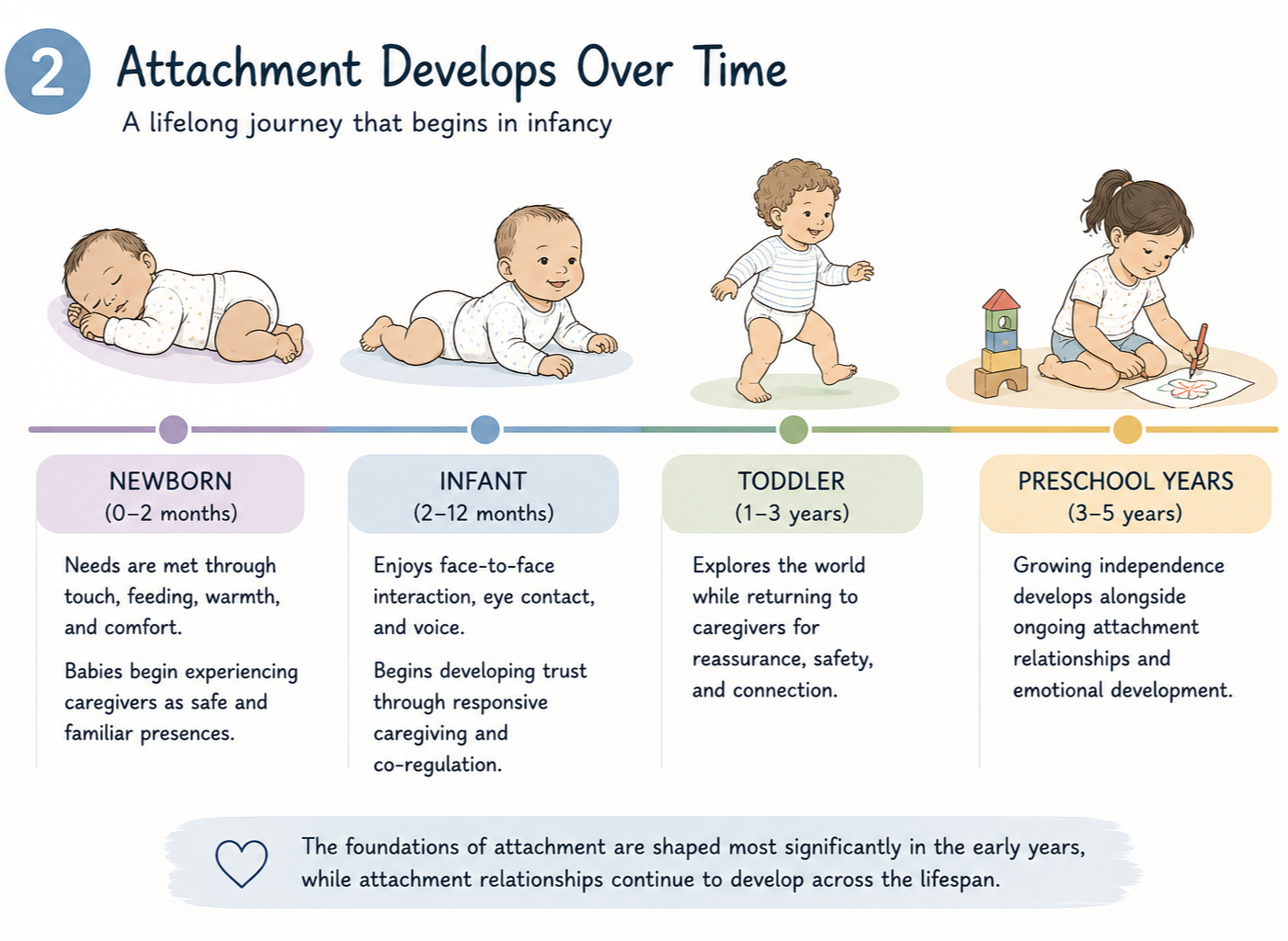
Attachment theory centres on infancy and early caregiving relationships. It describes the emotional bonds newborn babies and infants develop with the people who consistently care for them in early life.
Originally developed by John Bowlby in the mid-20th century, attachment theory initially focused heavily on the relationship between a baby and their mother, with early theory suggesting that attachment patterns were largely established within the first three to five years of life.
Contemporary understanding has since evolved considerably. Attachment is now understood as more relational, culturally informed, and adaptable across the lifespan. While the foundations of attachment are shaped most significantly during infancy and the early years, particularly from birth to around five years, attachment relationships continue to develop and change throughout childhood, adolescence, and adulthood through ongoing relational experiences.
Modern attachment theory also recognises that babies may form strong attachment relationships with a range of consistent caregivers, including parents, grandparents, kinship carers, foster carers, siblings, and other significant adults involved in their care. This broader understanding better reflects the many ways caregiving occurs across families, communities, and cultures worldwide.
Attachment is now understood to develop through responsive, emotionally safe, and consistent caregiving relationships rather than through one specific caregiver alone.
This understanding also includes premature and medically vulnerable babies, where attachment may develop through touch, voice, scent, skin-to-skin contact, emotional attunement, and responsive caregiving, even when early hospitalisation or separation has occurred.
Early Relational Development
Early psychoanalytic and object relations theorists, including Melanie Klein and Donald Winnicott, explored how newborn babies initially experience caregiving through the meeting of physical and emotional needs such as feeding, warmth, comfort, touch, and relief from discomfort. Through these repeated caregiving experiences, babies gradually begin to experience the caregiver not only as someone who meets their needs, but also as a safe and trusted relational presence.
Over time, babies increasingly seek emotional connection through eye contact, facial expression, voice, rhythm, touch, and attunement. These early relational experiences contribute to the development of safety, trust, emotional connection, and attachment.
Research in infant development and neurobiology has continued to expand understanding of the importance of relational attunement, co-regulation, gaze, facial expression, and caregiver responsiveness in early emotional development.


Secure Attachment
Secure attachment develops when babies and young children experience caregiving relationships that are responsive, emotionally available, and predictable most of the time.
Secure attachment is associated with:
Increased emotional safety and trust
Greater confidence to explore and learn
Stronger social and relational development
Improved emotional awareness and coping skills
Greater resilience during stress and change
Secure attachment does not mean a baby or child never becomes distressed or dysregulated. Rather, it reflects the experience of having relationships that feel safe enough to return to for comfort, support, and connection.
Insecure Attachment Patterns
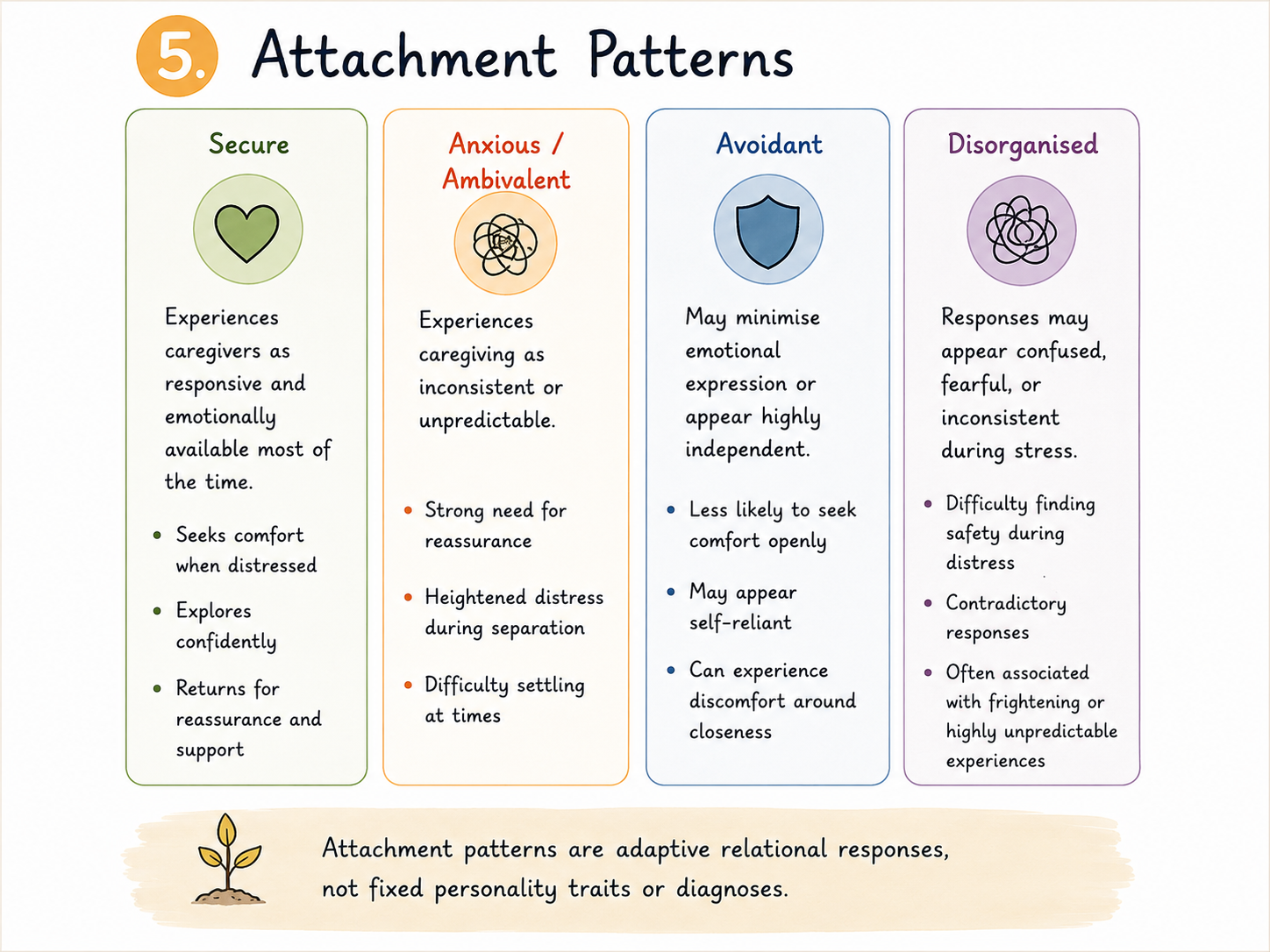
Some babies and children may develop protective attachment patterns when caregiving experiences are inconsistent, emotionally unavailable, frightening, or unpredictable. These responses are understood as adaptive survival responses rather than intentional behaviour.
Common attachment patterns include:
Anxious / Ambivalent Attachment
Avoidant Attachment
Disorganised Attachment
Importantly, attachment difficulties or disrupted early relationships do not automatically mean a child will develop an attachment disorder. Severe attachment disorders such as Reactive Attachment Disorder (RAD) and Disinhibited Social Engagement Disorder (DSED) are considered rare and are typically associated with significant neglect, severe relational trauma, institutionalisation, or highly disrupted caregiving environments in early childhood.
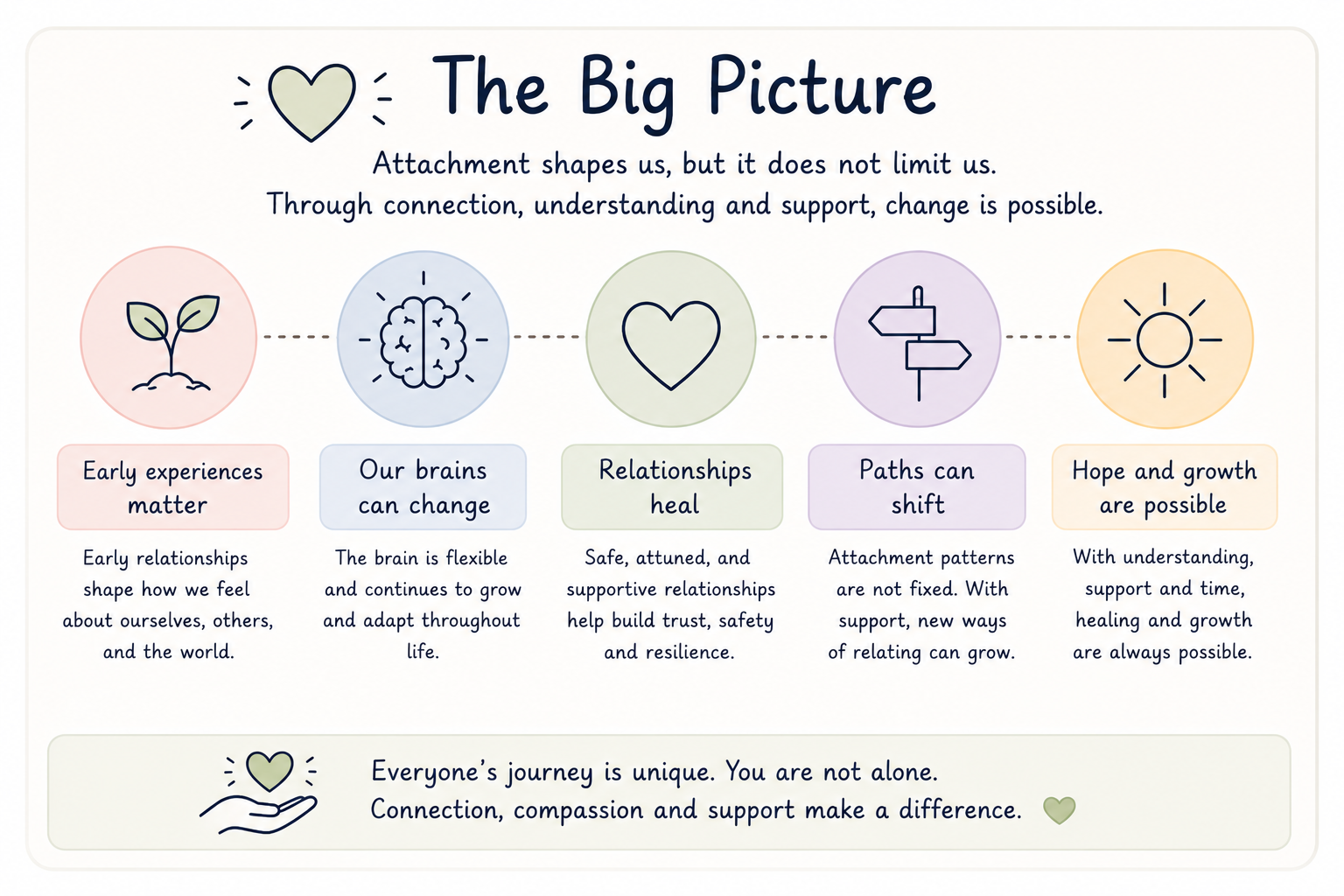
Contemporary understanding also recognises that attachment experiences are influenced by neurodevelopment, disability, trauma, sensory differences, caregiver stress, social context, culture, and broader life experiences. Attachment patterns are not fixed labels and can change over time through supportive, emotionally safe, and responsive relationships.

Disrupted or insecure attachments are relatively common and can occur when early caregiving relationships are inconsistent, stressful, disrupted, or emotionally unavailable. These experiences may affect how a child experiences safety, trust, emotions, and relationships, but do not mean a child has an attachment disorder. Attachment disorders, as defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, are rare and are typically associated with severe neglect, deprivation, or highly disrupted early care. Most children with attachment difficulties, trauma histories, or emotional and relational challenges do not meet criteria for an attachment disorder.
Attachment Across the Lifespan
Although attachment theory originally focused primarily on infancy and the early years, attachment relationships continue to evolve throughout life. Childhood experiences remain important, but later relationships, therapy, caregiving experiences, community connection, and emotionally safe relationships can all support healing, growth, and relational change over time.
Children and adults do not need perfect caregivers or perfect relationships. What matters most is the ongoing experience of safety, responsiveness, repair, and emotional connection within relationships.
Why Attachment Matters
Understanding attachment can help us better understand how babies, children, and young people experience safety, relationships, communication, learning, emotional development, and connection with others.
Attachment theory continues to provide an important foundation for supporting children and young people in ways that are relational, developmentally informed, and responsive to their individual needs. Rather than viewing behaviour in isolation, attachment-informed approaches encourage us to consider the child’s experiences, relationships, emotional safety, strengths, and environment as a whole.
This understanding underpins my own approach to creative arts psychotherapy and specialist learning support. Through relational, creative, and more-than-verbal approaches, I aim to support children and young people in developing emotional safety, confidence, communication, connection, learning engagement, and meaningful participation across home, school, and community environments.
Sam Gummer
MAAT, PGCE, BAHons
References
John Bowlby (1969/1982). Attachment and Loss: Volume I: Attachment. New York: Basic Books.
Mary Ainsworth, Blehar, M., Waters, E., & Wall, S. (1978). Patterns of Attachment: A Psychological Study of the Strange Situation. Hillsdale, NJ: Erlbaum.
Donald Winnicott (1965). The Maturational Processes and the Facilitating Environment. London: Hogarth Press.
Melanie Klein (1952). “Some Theoretical Conclusions Regarding the Emotional Life of the Infant.” In Developments in Psychoanalysis. London: Hogarth Press.
Daniel Stern (1985). The Interpersonal World of the Infant. New York: Basic Books.
Edward Tronick (2007). The Neurobehavioral and Social-Emotional Development of Infants and Children. New York: Norton.